

How To Perform The Double Calcaneal Osteotomy
The double calcaneal osteotomy includes a combination of the posterior calcaneal displacement osteotomy (PCDO) and the Evans anterior opening wedge calcaneal osteotomy. One would consider this combination for symptomatic flexible flatfoot deformity in both the adolescent flexible flatfoot and the adult with late stage II (Johnson and Strom’s classification) posterior tibial tendon dysfunction (PTTD). The PCDO consists of a transcortical osteotomy through the posterior tuber of the calcaneus with medial transposition of the tuberosity. The PCDO displaces the insertion of the Achilles tendon medially in relation to the subtalar joint axis, increasing the supinatory action during the midstance phase of gait. In addition, this procedure displaces the ground reactive forces medially in relation to the subtalar joint axis with medial translation of the plantar tubercle resulting in a supinatory moment at heel strike. The Evans anterior calcaneal osteotomy is placed approximately 1.0 cm proximal to the calcaneocuboid joint. The surgeon would subsequently place a laterally based wedge of bone into the osteotomy site, effectively lengthening the lateral column and stabilizing the midtarsal joint. The prevailing theory is that lengthening the lateral column creates a “bowstringing” effect that may be responsible for clinical restoration of the longitudinal arch. Lateral column lengthening will reduce inversion demand on the posterior tibial tendon and reduce the posterior muscle group force required to achieve the heel rise position. Surgeons may employ the double calcaneal osteotomy when significant calcaneal valgus, forefoot abduction and midtarsal joint instability coexist. The deformity must be flexible with no radiographic signs of tritarsal joint degeneration. The double calcaneal osteotomy is a joint sparing procedure that maintains a supple foot while restoring anatomic alignment, stabilizing the midtarsal joint and improving function.
What You Should Look For During The Physical Examination
Clinicians should evaluate the foot and ankle with both non-weightbearing and weightbearing exams. The examination should answer several key questions. Is the deformity flexible? What are the primary components of deformity (i.e., soft tissue contractures or muscle/tendon weakness)? What is the function of the tibialis posterior tendon? Does the ankle joint contribute to the valgus deformity? During the non-weightbearing exam, one should evaluate the ankle joint for the presence of instability, equinus, deformity or pain. Assess the tritarsal complex for flexibility and instability. Check for midtarsal joint instability by placing the subtalar joint in neutral and maximally loading the lateral column. When evaluating adult patients, one should check the course of the tibialis posterior tendon for tenderness, edema, nodularity or gross attenuation. Keep in mind that the tibialis posterior tendon is often unable to support the medial arch adequately in mid- to late-stage II PTTD and one may need to address this following osseous realignment. During the weightbearing exam, one should evaluate the frontal plane position of the calcaneus to the ground from a posterior view and observe any collapse of the longitudinal medial arch as well as any forefoot abduction. Reassess the hindfoot and midfoot flexibility in the weightbearing position by performing a hallux raise test with the patient standing. Dorsiflexing the hallux will recreate the longitudinal medial arch and reduce some calcaneal valgus as the tibia is forced to externally rotate in a reducible deformity. Clinicians should also evaluate the function of the tibialis posterior tendon in the weightbearing position using the double- and single-toe heel rise. The patient may be unable to perform a single heel raise in late stage II PTTD. Calcaneal osteotomies are contraindicated if the subtalar joint is non-reducible.
Pertinent Points On Diagnostic Imaging
Assess standard weightbearing views (AP, lateral and oblique views of the foot and ankle) for degenerative changes and angular deformity. Evaluating ankle films helps in ruling out a valgus deformity within the ankle joint. One can measure the talo-first metatarsal angle on AP and lateral foot radiographs. Obtaining a hindfoot alignment view and long leg calcaneal axial views can help in determining the level of valgus deformity (STJ vs. AJ vs. calcaneus). When assessing adolescent patients, clinicians should rule out tarsal coalitions. Obtaining a MRI can be helpful to rule out fibrous or cartilaginous coalitions in these patients. Advanced imaging is also beneficial to evaluate joint integrity when deciding between joint sparing procedures or an arthrodesis.
Key Pearls On Surgical Technique
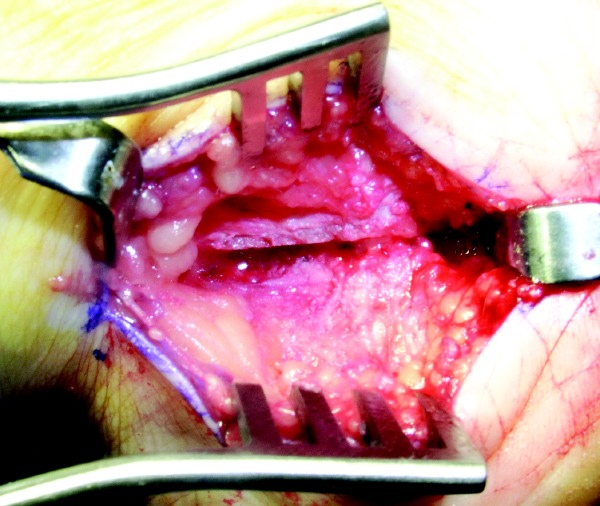
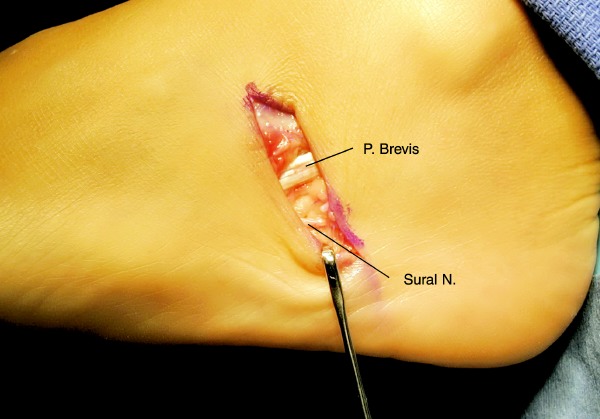
One should begin by placing the patient in the supine position on the operating table with a bump under the ipsilateral hip, placing the knee in the frontal plane to allow access to the lateral and medial hindfoot if medial tendon procedures are indicated. One may use spinal or general anesthesia. Prep the leg to the knee and drape the limb so you may access the posterior leg if a gastrocnemius recession or Achilles tendon lengthening is required. Place the incision for the PCDO on the posterior lateral aspect of the heel, beginning at a point approximately 2 cm anterior to the Achilles tendon and 1 cm posterior to the tip of the lateral malleolus. Extend the incision at a 45 degree angle toward the weightbearing surface in an anterior distal direction to a point just inferior to the calcaneal border. The incision remains posterior to the peroneal tendons. Incise the periosteum in the same fashion as the skin incision. Proceed with subperiosteal dissection to facilitate access for the sagittal saw. Dorsal dissection should reach just posterior to the posterior facet of the subtalar joint and inferiorly just anterior to the plantar tubercle. Hold the blade of the saw perpendicular to the lateral surface of the calcaneus and perform the osteotomy from lateral to medial. Use both hands to control the depth of the saw when approaching the medial cortex. Alternatively, you may use an osteotome to cut through or break the medial cortex. Place an osteotome within the osteotomy and stretch the medial periosteum. One may also utilize a lamina spreader to open and close the osteotomy completely, and stretch the medial periosteum. This maneuver will mobilize the tuber segment of the calcaneus and allow easy medial translation. Proceed to displace the posterior tuber medially and obtain provisional fixation with a 0.062 Kirschner wire or the guide wires for cannulated screw fixation. Hold the foot in plantarflexion during displacement in order to relax the inferior muscles, Achilles tendon and plantar fascia. This avoids sagittal plane displacement and allows for easy medial manipulation of the posterior segment. Translate the calcaneus approximately 1 cm medial. One should obtain a calcaneal axial view to ensure that you have achieved adequate correction. Achieve final fixation with one or two large diameter compression screws, and do not violate the subtalar joint. Osteosynthesis should be performed percutaneously under image intensification. One may choose to perform an osteoplasty of the remaining cortical shelf to avoid prominence. This will eliminate tension on the wound and avoid dehiscence. Adolescents with an open growth plate will require two smooth 5/64 in. or 7/64 in. Steinman pins, in lieu of screws, for final fixation. Surgeons may place these screws percutaneously or they may be buried. The incision for the Evans anterior calcaneal osteotomy is oblique or longitudinal, and made just distal to the sinus tarsi and 1 to 1.5 cm proximal to the calcaneocuboid joint (CCJ). Sometimes this can be deceiving if the plantar fat pad is laterally displaced. One must ensure careful dissection and preservation of the peroneal tendons and the sural nerve. It is important to identify the CCJ so one can avoid dissecting the periarticular structures that provide stability to this joint. Surgeons should perform the osteotomy approximately 1 cm proximal to the CCJ. Proceed to incise the periosteum in a vertical fashion. Avoid extensive plantar dissection and do not dissect the periarticular ligaments of the CCJ. This will prevent disruption of the long plantar ligament (LPL), which can result in an unstable distal segment following the osteotomy. This is not an uncommon radiographic finding following this procedure. Keep in mind that this still can occur depending on the size of the bone graft and stretch on the LPL. Ensure that the sagittal saw blade is angled just anterior to approximate the area in between the anterior and middle facets. One would also keep the osteotomy perpendicular to the weightbearing surface. Use caution when approaching the medial cortex. Exiting too far medially may compromise vital medial structures. It can sometimes be difficult to appreciate the medial cortex in this subchondral region of the calcaneus. One may use an osteotome to finish the osteotomy.
Essential Points On Using Bone Graft
Surgeons may employ a lamina spreader to distract the osteotomy. Alternatively, one may use a mini external fixator. One should evaluate the foot with the subtalar joint in neutral position and the forefoot loaded. Distract the osteotomy to the desired position and assess this position under image intensification. This will also help determine the size of bone graft needed. We prefer freeze-dried or frozen allograft bone for distraction. The allograft should be a composite of cortical bone to maintain structural realignment and cancellous bone to promote osteoconduction. Tricortical or bicortical iliac crest or patella grafts are ideal. Fashion the graft into a triangular shape with the base lateral. Place the graft into the osteotomy site. Using a mallet and tamp, tap the graft into position under tension. Increased tension will eliminate micromotion at the host-graft interface and promote consolidation. One should employ image intensification in order to verify the final placement of the graft. The graft size is usually 10 mm in width. However, you would use a larger graft for large individuals or if there is a significant deformity. We occasionally use fixation. The tension within the osteotomy invariably provides inherent stability. However, surgeons may apply a Kirschner wire, screw or small plate as a form of fixation to stabilize the sagittal plane position of the bone graft and the distal fragment.
In Conclusion
The double calcaneal osteotomy is a powerful procedure to correct calcaneal valgus, forefoot abduction and midtarsal joint instability in the adolescent flexible flatfoot or late-stage II PTTD among adults. Adjunctive soft tissue procedures may be indicated. Dr. Catanzariti is the Director of the Residency Training Program within the Division of Foot and Ankle Surgery at the Western Pennsylvania Hospital in Pittsburgh, Pa. He is a Fellow of the American College of Foot and Ankle Surgeons. Dr. Mendicino is Chief of the Division of Foot and Ankle Surgery at the Western Pennsylvania Hospital. He is a Fellow and Past President of the American College of Foot and Ankle Surgeons, and a Clinical Professor of Surgery at the Temple University School of Medicine Western Campus. Dr. Neerings is a Chief Surgical Resident within the Division of Foot and Ankle Surgery at the Western Pennsylvania Hospital in Pittsburgh, Pa. CE Exam #126 Choose the single best response to each question listed below: 1. The double calcaneal osteotomy is … a) not indicated for adolescents with symptomatic flexible flatfoot deformity. b) not indicated when there is coexisting forefoot abduction, midtarsal joint instability and significant calcaneal valgus. c) indicated for nonreducible deformity with radiographic evidence of degenerative joint disease. d) indicated for coexisting calcaneal valgus, forefoot abduction and midtarsal joint instability in the adolescent flexible flatfoot or late-stage II posterior tibial tendon dysfunction in adults. e) none of the above 2. During the clinical exam, one should evaluate the ankle joint for the presence of … a) equinus b) valgus c) pain d) instability e) all of the above 3. When evaluating adult patients, one should check the course of the tibialis posterior tendon for … a) tenderness b) edema c) nodularity d) gross attenuation e) all of the above 4. Obtaining a hindfoot alignment view and long leg calcaneal axial views can help determine … a) if there are any degenerative changes. b) the presence of fibrous coalitions in adolescent patients. c) the level of valgus deformity. d) all of the above e) none of the above 5. Obtaining an MRI can be helpful in ruling out … a) degenerative changes in adult patients. b) fibrous or cartilaginous coalitions in adolescent patients. c) fibrous or cartilaginous coalitions in adult patients. d) all of the above e) none of the above 6. One would place the incision for the PCDO on the posterior lateral aspect of the heel, beginning at a point approximately … a) 2 cm anterior to the Achilles tendon and 1 cm posterior to the tip of the lateral malleolus. b) 1 cm anterior to the Achilles tendon and 1 cm posterior to the tip of the lateral malleolus. c) 1 cm anterior to the Achilles tendon and 3 cm posterior to the tip of the lateral malleolus. d) 2 cm anterior to the Achilles tendon and 2 cm posterior to the tip of the lateral malleolus. e) None of the above 7. During the procedure for the PCDO, holding the foot in plantarflexion during displacement … a) ensures sagittal plane displacement. b) facilitates easy medial manipulation of the posterior segment. c) relaxes the inferior muscles, Achilles tendon and plantar fascia. d) a and b e) b and c 8. Which of the following answers is false? The development of an unstable distal segment following the Evans anterior calcaneal osteotomy … a) is not an uncommon radiographic finding after this procedure has been performed. b) is likely to occur regardless of the bone graft size. c) may be prevented by avoiding extensive plantar dissection and dissection of the periarticular ligaments of the calcaneocuboid joint. d) may occur depending on the size of the bone graft and stretch on the long plantar ligament. e) none of the above 9. When it comes to distracting the osteotomy in order to place the bone graft, the authors … a) prefer freeze-dried or frozen allograft bone. b) say patella grafts should be avoided due to concerns about osteoconduction. c) say the freeze-dried or frozen allograft bone should be a composite of cortical bone to promote osteoconduction and cancellous bone to maintain structural alignment. d) say bicortical iliac crest should be avoided due to concerns about maintaining structural alignment. e) none of the above Instructions for Submitting Exams Fill out the enclosed card that appears on the following page or fax the form to the NACCME at (610) 560-0502. Within 60 days, you will be advised that you have passed or failed the exam. A score of 70 percent or above will comprise a passing grade. A certificate will be awarded to participants who successfully complete the exam. Responses will be accepted up to 12 months from the publication date.
References:
1. Catanzariti AR, Lee MS, Mendicino RW: Posterior calcaneal displacement osteotomy for adult acquired flatfoot. J Foot Ankle Surg, 39(1): 2-14, 2000.
2. Catanzariti A: Medial displacement osteotomy of the posterior calcaneus for flatfoot deformity. Pediatric Foot and Ankle Deformity, edited by R. Jay, WB Saunders Co, Philadelphia, PA, 1999.
3. Den Hartog BD: Flexor digitorum longus transfer with medial displacement calcaneal osteotomy. Biomechanical rationale. Foot Ankle Clin, 6(1): 67-76, vi, 2001.
4. Dollard MD, Marcinko DE, Lazerson A, Elleby DH: The Evans calcaneal osteotomy for correction of flexible flatfoot syndrome. J Foot Surg, 23(4): 291-301, 1984.
5. Evans D: Calcaneo-valgus deformity. J Bone Joint Surg 57B: 270-278, 1975.
6. Frankel JP, Turf RM, Kuzmicki LM: Double calcaneal osteotomy in the treatment of posterior tibial tendon dysfunction. J Foot Ankle Surg, 34(3): 254-61, 1995.
7. Guyton GP, Jeng C, Krieger LE, Mann RA: Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: a middle-term clinical follow-up. Foot Ankle Int, 22(8): 627-32, 2001.
8. Johnson KA, Strom DE: Tibialis posterior tendon dysfunction. Clin Orthop, (239): 196-206, 1989.
9. Koutsogiannis E: Treatment of mobile flat foot by displacement osteotomy of the calcaneus. J Bone Joint Surg 53B: 96-100, 1971.
10. Martin DE, Stran DC, Southerland JT, Wesselowski BE: Callus distraction in reconstructive foot surgery, JFAS, 35: 489-506, 1996.
11. Mendicino SS: Posterior tibial tendon dysfunction. Diagnosis, evaluation, and treatment. Clin Podiatr Med Surg, 17(1): 33-54, vi, 2000.
12. Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot. Results in children who had severe, symptomatic flatfoot and skewfoot. JBJS Am, 77: 500-512, 1995.
13. Moseir-LaClair S, Pomeroy G, Manoli A: Intermediate follow-up on the double osteotomy and tendon transfer procedure for stage II posterior tibial tendon insufficiency. Foot Ank Int 22(4): 283-291, 2001.
14. Mosier-LaClair S, Pomeroy G, Manoli A, 2nd: Operative treatment of the difficult stage 2 adult acquired flatfoot deformity. Foot Ankle Clin, 6(1): 95-119, 2001.
15. Myerson MS, Corrigan J: Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon transfer and calcaneal osteotomy. Orthopedics, 19(5): 383-8, 1996.
16. Myerson MS, Corrigan J, Thompson F, Schon LC: Tendon transfer combined with calcaneal osteotomy for treatment of posterior tibial tendon insufficiency: a radiological investigation. Foot Ankle Int, 16(11): 712-8, 1995.
17. Phillips GE: A review of elongation of os calcis for flat feet. JBJS, 65b(1): 15-18, 1983.
18. Pomeroy GC, Manoli A, 2nd: A new operative approach for flatfoot secondary to posterior tibial tendon insufficiency: a preliminary report. Foot Ankle Int, 18: 206-212, 1997.
19. Raines RA Jr., Brage ME: Evans osteotomy in the adult foot: an anatomic study of structures at risk. Foot Ankle Int, 19: 743-747, 1998.
20. Saltzman CL, el-Khoury GY: The hindfoot alignment view. Foot Ank Int 16:572-76, 1995.
21. Sung IH, Lee S, Otis JC, et al: Posterior tibial tendon force requirement in early heel rise after calcaneal osteotomies. Foot Ank Int 23(9): 842-849, 2002.
22. Weil LS Jr., Roukis TS: The calcaneal scarf osteotomy: operative technique. J Foot Ankle Surg, 40(3): 178-82, 2001.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}